Skin is our largest organ, made up of complex sensors constantly monitoring for anything that might cause us pain. Our new technology replicates that – electronically.
The electronic artificial skin we’ve developed reacts to pain stimuli just like real skin, and paves the way for better prosthetics, smarter robotics and non-invasive alternatives to skin grafts.
Our prototype device mimics the body’s near-instant feedback response and can react to painful sensations with the same lighting speed at which nerve signals travel to the brain.
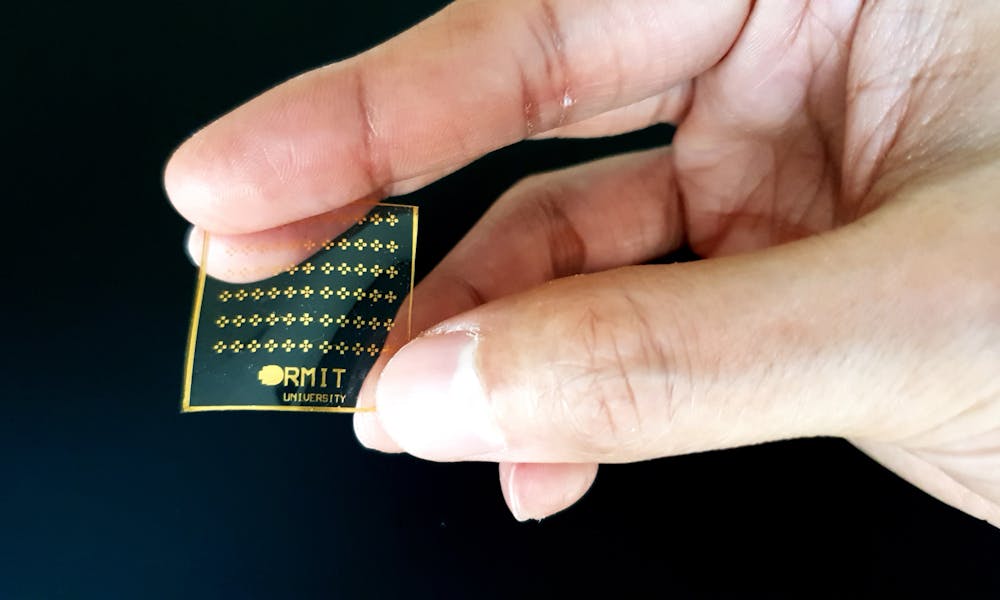
Our new technology, details of which are published in Advanced Intelligent Systems, is made of silicone rubber with integrated electronics. It mimics human skin, both in texture and in how it responds to pressure, temperature and pain.
Human skin senses things constantly, but our pain response only kicks in at a certain threshold. Once this threshold is breached, electric signals are sent via the nervous system to the brain to initiate a pain response.
You don’t notice when you pick up something at a comfortable temperature. But touch something too hot, and you’ll almost instantly recoil. That’s our skin’s pain-sensing system in action.
Helping hand
Our new pain-sensing electronic skin is a crucial step towards the development of “smart prosthetics” featuring sophisticated feedback systems. We want to develop medical devices and components that show similar pain sensing responses to the human body.
Prosthetics significantly improve an amputee’s quality of life, but they still lack the ability to sense danger. A prosthetic hand does not sense when it’s placed on a hot surface, while someone with a prosthetic arm might lean on something sharp but won’t realise the damage being caused.
Technology that provides a realistic skin-like response can make a prosthetic much more like a natural limb.
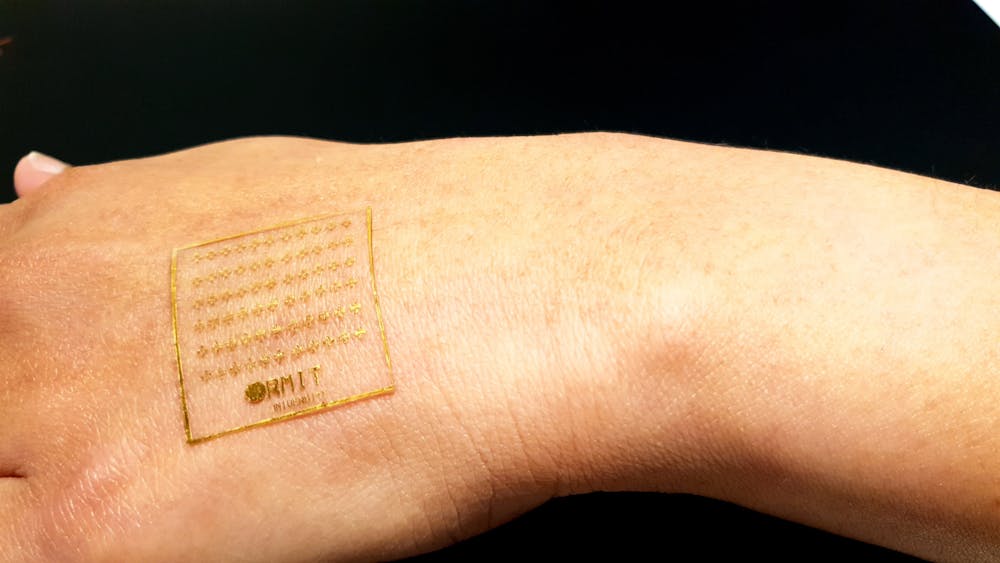
With further development, our electronic skin could also potentially be used for skin grafts, in cases where the traditional approach is not viable.
The new silicone skin could pave the way for smarter skin grafts. RMIT University, Author provided
For example, we used our process for integrating temperature-sensitive vanadium oxide, a material that can change its electronic behaviour in reaction to temperatures above a particular threshold (65℃ in this case).
This material then triggers electrical signals similar to those generated by our nerve endings when we touch something hot. The electrical signal from the sensing part of the system (which is temperature- or pressure-sensitive) goes to a brain-mimicking circuit which processes the input and makes a decision based on threshold values.
The electrical output from the brain-mimicking circuit is like the nerve signals that initiate a motor response (such as moving your hand away) in the human pain response.
In our experiment, we measured the current generated. To use the silicone skin for real, this would need to be connected to nerve endings or apparatus that could initiate a motor response.
Our material responds just as fast as a real human pain response, mimicking the entire process from stimulus to response triggers from the brain – or in our case, the brain-mimicking circuit. The response is stronger depending on both the intensity and time of stimulation – just like a real human pain response.
The electronic skin brings to reality the threshold-based responses to pain, both in the way the skin reacts differently to pain above a certain threshold and how it takes longer for skin to “recover” from something that’s more painful. This is because stronger stimuli generate more voltage across the brain-mimicking circuit.
We can also modify this threshold in our devices to mimic the way injured skin (such as sunburnt skin) can have a lower pain threshold than normal skin. The electronic skin can also be used to increase sensitivity, which could be particularly useful in sports and defence as well as for skin grafts.
Another unique application could be smart gloves that could provide precise feedback from a surgeon’s hands when palpating tissue.
Our silicone skin will need further development to integrate the technology into biomedical applications. But the fundamentals – biocompatibility and skin-like stretchability – are already there.
The next steps are working with medical researchers to make this even more “skin-like”, and to figure out how best to integrate it with the human body.
Regularly and thoroughly washing your hands with soap and water for at least 20 seconds, or using an alcohol-based hand sanitiser, are key steps to reducing the risk.
But with all this hand washing, it’s easy to get dry skin or for existing skin conditions to flare up.
The top layer of our skin (the stratum corneum) is our skin’s key protective layer. But frequent hand washing with repetitive exposure to water, soap and skin cleansers will disrupt this layer.
Over time, this leads to dry skin, further disruption of the skin barrier and inflammation.
Irritant contact dermatitis is more common in people who perform “wet work” as they wash and dry their hands many times a day.
They include health-care workers (doctors, nurses, personal care assistants), hairdressers, food handlers, kitchen staff and cleaners. They may also be exposed to irritating skin cleansers and detergents.
But now handwashing is becoming more frequent during the COVID-19 pandemic, there may be more affected people outside these occupations.
Health-care workers, who wash their hands multiple times a day, are particularly at risk of hand dermatitis. Shutterstock
People with eczema, asthma and hay fever are also at higher risk of developing irritant contact dermatitis or experiencing a flare of underlying eczema.
People with eczema or who have had contact dermatitis before will have more easily irritated skin. While they can still use hand sanitisers, it’s recommended they wash with gentler soap-free washes rather than normal soap.
Soap-free washes contain non-soap-based synthetic detergents (syndets). Syndets have a nearly identical cleansing action as soap, but with the benefit of having the same pH as the skin. This means they’re less likely to remove the oils from the outer layer of the skin and are less irritating.
Soaps have a high pH and are quite alkaline. This disrupts the outer layer of the skin, allowing the soap to penetrate deeper into the skin, thus causing more skin irritation and itching.
Other people who don’t have eczema or a history of contact dermatitis should just use soap. Liquid soaps usually contain fragrances and preservatives, which can cause another type of dermatitis (allergic contact dermatitis), so opt for a plain, unperfumed bar soap.
2. Dry your hands thoroughly
Dry your hands thoroughly, including the webs of your fingers and under your
rings to reduce dermatitis caused by trapped water. Skin irritation and breakdown can occur when there is excessive moisture, soap residues and water trapped between the skin and underneath rings.
Moisturisers come in different formulations. While lotions are light in consistency and convenient to use during the day, they will require more frequent applications. Creams and ointments have thicker and oilier texture, are effective for dry hands and are best used overnight.
Fragrances can cause allergic contact dermatitis and are best avoided, where possible.
4. Use alcohol-based hand sanitiser (if you can get hold of it)
Alcohol-based hand sanitiser will reduce your skin’s contact with water, and so lower your risk of dermatitis.
Research in health-care workers shows hand sanitisers cause less contact dermatitis than washing with soap and water.
Sometimes people wrongly believe that when hand sanitiser stings on a paper cut, this means that they are allergic. But this is an irritant reaction and though uncomfortable, it’s safe to keep using it.
Which sanitiser? This usually comes down to personal preference (and what you can get hold of).
5. Use gloves
Use protective gloves when doing household chores, such as washing the dishes or when gardening.
Use cotton gloves when doing dry work, such as sweeping or dusting, to protect your hands and minimise the need to wash them.
Use washing up gloves where possible. Shutterstock
At night, moisturise your hands than wear cotton gloves. This acts like an intensive hand mask and works wonders for very dry skin. It ensures the moisturiser stays on your hands and increases its penetration into your skin.
What if my hands are already damaged, dry or cracking?
1. Act early
Treat hand dermatitis as soon as it occurs, otherwise it will get worse.
2. Apply petroleum jelly
If you think you’ve lost your nail cuticle (the protective barrier between the nail and nail fold), water will be able to seep into the nail fold, causing swelling and dermatitis.
Use petroleum jelly, such as Vaseline, as a sealant to prevent further water damage. Petroleum jelly can also be used on skin cracks for the same reason.
3. Seek medical help
If there are any red, dry and itchy areas, indicating active dermatitis, seek help from your GP or dermatologist.
They can start you on a short burst of an ointment that contains corticosteroids until the rash subsides.
Prescription ointments are likely to be more effective than over-the-counter creams because of their higher potency.
But you could start with buying 1% hydrocortisone ointment, not cream, from the chemist.
Sometimes dermatitis can become infected with skin bacteria such as Staphylococcus aureus. Seek medical advice if you experience symptoms such as persistent soreness or pain.
You should also seek medical help if you have severe hand dermatitis not responding to home treatments.
Most GPs and dermatologists are moving to or have started using telehealth so you can consult them using a video call, minimising face-to-face appointments.
The itchiness of hives or urticaria can severely affect people’s quality of life, particularly if symptoms last or antihistamines don’t work. from www.shutterstock.com
Have you ever wondered who buys those huge boxes of antihistamines prominently displayed all year round in your local pharmacy? If antihistamines were just used for hay fever, you’d think sales would be good in spring, but pretty mediocre for the rest of the year.
Many of the antihistamines sold in Australia are actually for hives, or what doctors call urticaria. Hives produces multiple red, raised bumps (or wheals) that are incredibly itchy. Hives occurs all year round.
The condition is really common, with a Korean study showing around 22% of people can expect to have it at some time in their life.
Some people also get angioedema, where small blood vessels leak fluid into the tissues, causing spectacular swelling. If the swelling affects your throat and airways you can suffocate.
Fortunately, for the vast majority of people, hives comes and goes in a couple of weeks. While you can feel pretty miserable when you have it, antihistamines work well to control the rash and itch. Suffocation is exceptionally rare.
When hives won’t go away
If you are unlucky enough to still have hives after six weeks, it’s likely to persist six months, six years or even 26 years later.
This is what dermatologists call chronic urticaria, which affects about 1% of the population (around 250,000 Australians). The itch, sleep disturbance, swelling and rash associated with it severely impair people’s quality of life. Of all skin diseases, chronic urticaria seems to worsen your mood and disrupt day-to-day living the most.
One antihistamine tablet is usually enough to control hay fever. But people with chronic urticaria may need two, three or sometimes four tablets a day to control their itch. Even that may not be enough to stop the wheals.
What causes hives?
So what causes hives? If your hives go away within six weeks, you probably had them because of a delayed reaction to a viral infection. Sometimes this acute condition is caused by an allergic reaction to a medication; an antibiotic allergy is a common cause. Occasionally a food allergy causes hives.
What about chronic urticaria, when hives last more than six weeks? Doctors don’t know the exact cause. While patients often suspect a food allergy, doctors rarely find a food trigger.
We don’t know exactly what causes hives, seen here as raised, red bumps or wheals. from www.shutterstock.com
But we know autoimmunity is involved, when the body’s immune system targets itself.
Most patients with chronic urticaria have antibodies against their own immune system. In particular, these antibodies target molecules critical to a normal allergic response (immunoglobulin E, or IgE, and its receptor).
If antihistamines don’t help, there are other options.
Medications that specifically target IgE and get to the root cause of urticaria autoimmunity are now available, provided you meet all the special criteria. Only dermatologists are allowed to prescribe this medicine on the PBS.
To date, omalizumab has been the most effective treatment for chronic urticaria patients who don’t respond to antihistamines. It’s given as an injection under the skin every four weeks. Unfortunately symptoms in fewer than 50% of patients are completely controlled.
A new drug ligelizumab, which is still in clinical trials, is showing promise, according to international research we were involved with published recently in the New England Journal of Medicine. However, this experimental drug, which also targets IgE autoimmunity, is only available in Australia as part of a clinical trial.
There’s a lot to be said for sunshine – both good and bad. It’s our main source of vitamin D, which is essential for bone and muscle health. Populations with higher levels of sun exposure also have better blood pressure and mood levels, and fewer autoimmune diseases such as multiple sclerosis.
On the other hand, excess UV exposure is estimated to contribute to 95% of melanomas and 99% of non-melanoma skin cancers. These skin cancers account for a whopping 80% of all new cancers each year in Australia.
Like any medicine, the dose counts. And in Australia, particularly in the summer, our dose of UV is so high that even short incidental exposures – like while you hang out the washing or walk from your carpark into the shops – adds up to huge lifetime doses.
Fortunately, when it comes to tanning, the advice is clear: don’t. A UV dose that’s high enough to induce a tan is already much higher than the dose needed for vitamin D production. A four-year-long study of 1,113 people in Nambour, Queensland, found no difference in vitamin D levels between sunscreen users and sunscreen avoiders.
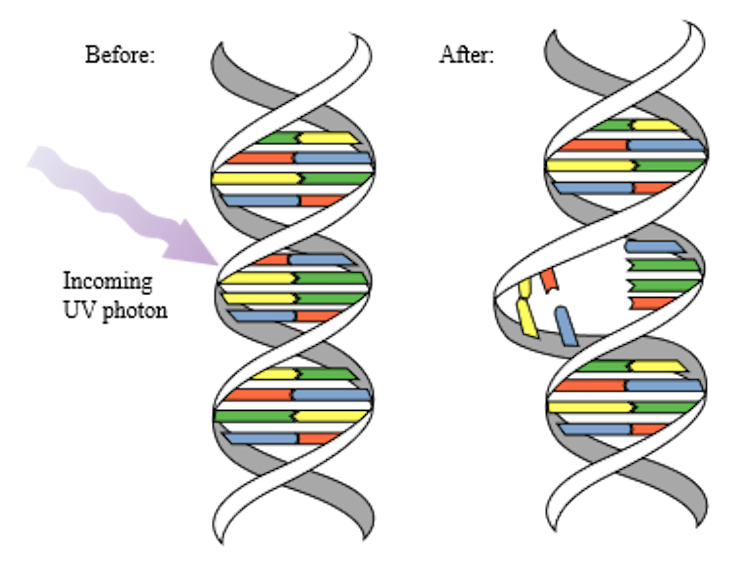
A tan forms when ultraviolet (UV) rays from the sun discharge too much energy into our skin, causing damage to membranes, proteins, and most importantly, DNA. The excess energy of UVB rays (part of the UV ray that penetrates the upper layers of our skin) prevents the DNA from copying correctly when the cells multiply which can cause mutations.
UVA rays which penetrate deeper into the skin can trigger a reactive and harmful process (known as oxidative free radical damage) which can damage not just DNA but also many of the skin’s structural components. It’s been estimated a single day’s sun exposure can cause up to a million DNA defects in each skin cell.
Excess energy from UVB rays causes DNA bases to link up incorrectly, making it difficult to copy accurately and leading to mutations that can cause cancer. NASA/David Herring
Once their DNA repair mechanisms detect large amounts of damage, skin cells signal pigment-producing cells (melanocytes) to start producing extra melanin, the pigment that gives our skin, hair and eyes their colour.
The extra melanin is parcelled up and transported into other skin cells to settle over and protect the part of the cell containing the DNA. This filters some UV rays and gives tanned skin its brown colour. But this tan doesn’t provide much help – it’s only as protective as SPF 2 sunscreen.
Two in three Australians will develop a skin cancer in their lifetime, mostly thanks to the DNA damage caused by UVB rays. But premature ageing is a less well-known effect of too much sun exposure.
UVA rays penetrate deep into the dermis, the lower layer of the skin, and generate reactive oxygen that damages the skin’s structures. Over time this causes solar elastosis, where irregularly thickened clumps of elastic fibres form, then degrade into disorganised, tangled structures.
This 70-year-old has deep wrinkling and skin darkening caused by long-term sun exposure on her neck and part of her chest exposed by her shirt, while the rest of her skin has stayed relatively clear and unwrinkled. Author provided
Eventually this can take the form of roughening or leathery appearance, deep wrinkling, dark blotches and star-shaped white patches, and an overall yellowish tone. Prematurely-aged skin is often more easily-bruised or has broken capillaries.
Dark blotches and white scar-like patches are common signs of ageing caused by too much sun. DermNetNZ.org
But I like the way a tan looks. What now?
It’s well known that a tanned look seems healthy and attractive to many Australians. Recent research shows Australians who feel particularly self-conscious about their body are more likely to intentionally tan to increase their sense of attractiveness.
Fortunately, there’s a safe way to indulge in the aesthetics of golden-brown skin: any tan that comes out of a bottle with the active ingredient dihydroxyacetone. This is a colourless sugar molecule that turns brown when it reacts with amino acids in the skin. It’s safe to use because it doesn’t penetrate deeper than the very top layer of skin, where the cells are already dead.
Don’t be tempted by solariums and sunbeds, because they emit up to six times as much UV as the midday summer sun. Commercial solariums are illegal in Australia for this reason, but there are still privately-owned sunbeds in use. Avoid them at all costs.
So how do I stay sun safe without living in a cave?
There are two parts to sunsafe behaviour in Australia that lets you get the health benefits of sunshine and prevents you from being one of the 2.4 million Aussies getting sunburnt each weekend.
First, you should wear 30+ SPF sunscreen every day when the UV index in your area is three or higher. By putting it on everywhere that isn’t covered by that day’s outfit, you protect yourself from the damage accumulated by short exposures, day in and day out, in Australia’s intense UV environment.
You should make sunscreen part of your morning routine, like brushing your teeth. Use the Cancer Council’s free Sun Smart app or check your local weather report to find out the UV index where you are today.
During the cooler months in southern parts of Australia, when the UV index is often below three, it’s good to spend some time on most days, in the middle of the day, with skin exposed to the sun to maintain healthy vitamin D levels.
So, a lunchtime stroll with your sleeves rolled up is a good idea in July in Hobart, where the UV index only gets up to one. In Brisbane at the same time, with an average July UV index of four, you don’t need to take special steps to get enough vitamin D.
Second, if you’re planning to be outside for a prolonged time, you should follow the Slip Slop Slap Seek Slide advice. Slip on a long-sleeved shirt, slop on sunscreen, slap on a hat, seek shade and slide on some sunglasses. Reapply your sunscreen every two hours, and be sure to use plenty: you want about a teaspoon each for your back, chest, head/neck, and each arm and leg.
This article is part of our series about skin: why we have it, what it does, and what can go wrong. Read other articles in the series here.
Dermatological emergencies are uncommon, but can cause devastating complications and death if not recognised and treated early. Some skin conditions require treatment in an intensive care unit. Here are some of the most serious skin conditions and what you should know about recognising them.
1. Necrotising fasciitis
Necrotising fasciitis is a severe infection of the skin, the tissue below the skin, and the fascia (fibrous tissue that separates muscles and organs), resulting in tissue death, or necrosis. The infection is rapid, fast-spreading and fatal if not detected and treated early. If not treated with antibiotics and surgery early, toxic shock and organ failure are common.
Necrotising fasciitis may occur in anyone. Previously healthy young people are often affected.
The cause may be one or more bacteria entering the body via an external injury or punctured internal organ. Group A streptococci bacteria, which are the organisms implicated in “strep throat”, are among the most common causes.
Early necrotising fasciitis is easily missed, as similar symptoms are commonly seen in less severe infection. The initial area is painful, red and swollen. This progresses to a dark, blistered, malodorous and blackened area, which is a sign of tissue death. Other symptoms include fever, intense pain, low blood pressure and shock.
The most important risk factors for necrotising fasciitis include diabetes, peripheral vascular disease, trauma, alcohol and intravenous drug use, and use of non-steroidal anti-inflammatory drugs.
Treatment of necrotising fasciitis is immediate hospitalisation, surgical removal of all dead tissue, and intravenous antibiotics. Patients often require intensive care. Management of shock and other complications reduces the risk of death. Use of a hyperbaric chamber (to increase oxygen delivery to the tissue) and immune therapy may also be required.
Most have heard of necrotising fasciitis as the ‘flesh-eating bug’. DermNet New Zealand
2. Scalded skin syndrome
Staphylococcal scalded skin syndrome is an uncommon major skin infection. It typically affects newborn babies, young children and adults with reduced immune systems or kidney failure. This syndrome is caused by toxins produced by the bacterium Staphylococcus aureus, which is common in throat, ear and eye infections.
Around 15-40% of adults carry Staphylococcus aureuson the skin surface and have no problems. But these adults may inadvertently introduce the bacteria into nurseries or daycare centres. Because young children have weak immunity to specific toxins, they’re at increased risk of scalded skin syndrome.
Scalded skin syndrome is characterised by a red, blistering rash resembling burns. Early symptoms include fever, skin redness and skin tenderness. Other symptoms may include sore throat or conjunctivitis.
Within 24-48 hours, fluid-filled blisters form on the entire body. The blisters may rupture, leaving areas resembling burns. Large areas of the skin peel off and fall away with only minor touch.
Scalded skin syndrome requires hospitalisation for intravenous antibiotics and treatment of the wounds. Ruptured blisters require wound dressings, and the skin surface requires intense care to avoid further damage.
Other treatment includes intravenous fluid and electrolyte maintenance to prevent shock and other complications, paracetamol for pain and fever, and avoidance of severe sepsis. Sepsis is when chemicals released into the bloodstream to fight an infection trigger inflammatory responses throughout the body, which can be life-threatening.
Complications of scalded skin syndrome include severe infection, pneumonia, cellulitis (a bacterial skin infection) and dehydration. Most children treated appropriately recover well and healing is complete within a week.
Staphylococcal scalded skin syndrome is more likely to occur in people with weaker immune systems – such as children. DermNet New Zealand
3. DRESS syndrome
Standing for “drug reaction with eosinophilia and systemic symptoms,” DRESS syndrome is a severe reaction that affects the skin and internal organs. The patient may have an extensive rash, fever, enlarged lymph nodes and damage to the liver, kidneys, lungs, heart, blood components or pancreas. Symptoms usually start two to eight weeks after the responsible drug has been taken.
The death rate is estimated between 10 and 20%, most often due to liver failure.
The most common drugs responsible include anticonvulsants, antidepressants, non-steroidal anti-inflammatory drugs, antibiotics and sulfa drugs (a type of synthetic antibiotic). The severe reaction is thought to occur due to a pre-existing genetic change in the immune system, a triggering illness (most often a viral infection) and defective breakdown of the drug by the body.
Early diagnosis is essential. The responsible drug must be stopped immediately and patients may require intensive care or burn unit management. More intensive treatment is needed if organs are involved.
DRESS syndrome appears a few weeks after taking a drug the patient is allergic to. DermNet New Zealand
4. Life-threatening drug reactions
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are variants of a life-threatening reaction that affects the skin and mucous membranes (mouth, eyes, genitals, respiratory or gastrointestinal tracts).
These are unpredictable reactions that leave sufferers critically unwell, with widespread death of the outer skin layer (epidermis), which peels off. The rash generally begins on the trunk and extends to the limbs and face, and there is intense skin pain. Before the rash appears, symptoms include fever, sore throat, runny nose, conjunctivitis and general aches.
It’s almost always caused by medications. The most common medications causing this reaction are anticonvulsants, antibiotics, allopurinol (gout medication), non-steroidal anti-inflammatory drugs and an HIV drug. The reaction usually occurs in the first eight weeks after taking the drug. It’s more likely to happen if the patient has cancer, HIV or specific genes that may play a role.
This reaction can be fatal by causing dehydration and malnutrition, severe infection, respiratory failure, gastrointestinal complications and multi-organ failure.
The responsible drug has to be stopped, and treatment (in a burns unit and intensive care unit) includes wound care, fluid management, pain management and prevention of infection. Long-term complications, including scarring, eye, oral, genital, lung disease and mental health disorders, are common. Around a quarter of people with this reaction will die.
This article is part of our series about skin: why we have it, what it does, and what can go wrong. Read other articles in the series here.
Everyone has had the unpleasant experience of a rash on the skin – pink, red or purple, flat or bumpy, itchy, scaly, pus-filled, or just plain unsightly. This variety isn’t surprising, because the skin is a complicated organ.
Infections, allergic reactions, immune system problems and even bad reactions to medication can all manifest as a rash.
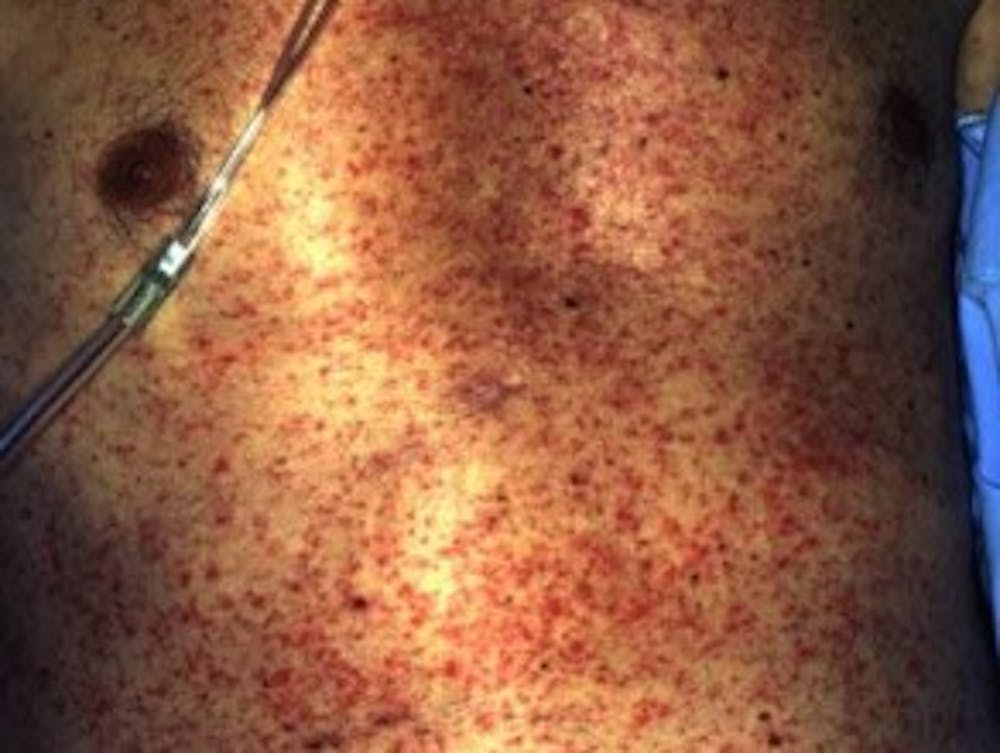
This rash usually appears within two weeks of starting a new medication, as a widespread, symmetrical rash with pink-to-red spots that are flat or elevated and firm, and that might join together in patches.
This type of rash is a hypersensitivity reaction, in which the attacking soldiers of the immune system (called “T-cells”) detect the drug and try to clear it from the body by releasing inflammatory proteins.
Exanthematous drug eruption. DermNet New Zealand.
Very rarely, a drug can cause a severe and life-threatening rash called “toxic epidermal necrolysis” where the skin begins to peel off in sheets. It’s more common in Han Chinese people with a specific genetic variant, and requires intensive care or burn unit treatment.
Most drug eruptions go away within a week once the patient stops taking the problem medication, or within several weeks in protracted cases. In the meantime, or if the drug is essential, steroid creams (which reduce inflammation) and emollient (softening) moisturisers can bring some relief.
Allergic contact dermatitis
Allergic contact dermatitis is caused by direct skin contact with a substance to which the person is allergic. The immune system’s T-cells overreact to the allergen and release proteins that call more immune cells to the area, making it red and swollen.
It’s often itchy and can be blistered or dry but bumpy. The reaction is often delayed by 48-72 hours, so it can be difficult to determine exactly what caused the reaction. It should also die down by itself over a few days, as long as the allergen is no longer on the skin.
Contact allergies can develop suddenly after years of exposure to an allergen. Jewellery containing nickel, fragrances in lotions, household cleaners, preservatives in hair products, and latex in gloves or condoms are common sources. A dermatologist can carry out a patch test to determine whether a substance is the allergen, by applying it to a small patch of skin.
Severe contact dermatitis from a drug patch. Dr. Khatmando
Active dermatitis is treated with emollient moisturisers and steroid creams, or with oral steroids or drugs to suppress the immune system if very severe. Further episodes can be prevented by becoming aware of the sources of the allergen, reading labels carefully, and using gloves to handle allergen-containing products.
Eczema
Atopic dermatitis or atopic eczema (often just called eczema) is very common in children from three months old onwards, but appears in adults too, often with hay fever and asthma.
Atopic dermatitis features patches of intensely itchy red skin, sometimes with blisters and weeping patches. Children often have open sores and scabs, because it’s so itchy that it’s hard to refrain from scratching.
Over time the skin becomes thickened and rough from frequent scratching and rubbing. Childhood atopic dermatitis tends to improve as the child grows up, but may continue. Far less commonly, atopic dermatitis can also appear first in adulthood.
Atopic dermatitis is very common in children, but often improves as they get older. DermNet New Zealand
Atopic dermatitis is a disease of the immune system, in which
structural defects in the skin barrier make it easier for irritants to penetrate into the skin. This throws the delicate balance of the microbial community on our skin out of whack, causing the immune system to go into overdrive. Triggers include stress, sweating, coarse fibres in clothing, inhalation of allergens such as pollen, irritants such as soap or perfumes, and eating food we’re allergic to.
Steroid creams can help treat a bad flare of atopic dermatitis, but shouldn’t be used constantly. In very severe cases, immunosuppressant drugs are prescribed. Ongoing control of atopic dermatitis often includes using emollient moisturisers to combat dry skin, keeping cool, avoiding hot water or irritants, and reducing allergens such as dust mites in the home.
For severe cases that don’t respond to these methods, the drug dupilumab has just been approved for use in Australia. This drug blocks a specific cell receptor to prevent immune cells from detecting two overactive inflammatory proteins.
Atopic dermatitis can have a big impact on quality of life, due to insomnia from the constant itchiness, and restrictions on clothing, body products, pets or activities. Its presence on prominent parts of the body like the face and hands can also reduce self-esteem. Evening sedatives to improve sleep and psychotherapy can help reduce the impact on everyday life.
Psoriasis
Psoriasis is another chronic immune disorder. It can start at any age and can be lifelong, and is usually present as red plaques (raised or thickened skin) with well-defined edges and silvery-white scales, ranging from a few millimetres to several centimetres across. The overactive inflammation can also damage the joints and lead to psoriatic arthritis.
Often the plaques feel itchy or sore, and because psoriasis is long-lasting and can appear prominently on highly visible parts of the body, it often comes with severe psychological effects.
Psoriasis lesions are raised, red and often have white scales. DermNet New Zealand
Psoriasis is caused by too many new skin cells being produced and moving up to the surface of the skin too quickly. It’s not known exactly why, but there’s usually an overabundance of inflammatory messenger proteins in the skin.
It can be triggered or aggravated by a streptococcal infection such as tonsillitis, smoking, hormonal changes such as menopause, and some medications. Genetics play an important role in susceptibility to psoriasis and also in what treatments are effective.
Chronic plaque psoriasis, the most common form, can be very resistant to treatment. Small areas can be treated with creams containing steroids, coal tar, or vitamin D. If a lot of the body is covered by plaques, oral immunosuppressant drugs are used, or phototherapy, which uses targeted UV light to destroy over-active immune cells. Moderate sun exposure sometimes improves psoriasis, but sunburn can worsen it – a tricky balance in Australia’s high-UV environment.
These treatments can usually improve the plaques, but it can be very difficult to clear it completely. There are several new drugs coming onto the market for severe psoriasis that hasn’t responded to other treatment.
Tinea
Tinea, or ringworm, is not caused by worms at all but a fungal infection. Tinea is usually named according to the body site it’s on, but the same few kinds of fungus can cause tinea in many parts of the body and it can be spread from one part of the body to another, such as by scratching or using a contaminated towel.
Tinea pedis, on the foot, is an important type because spores can live for weeks in communal showers and changing rooms, making it a common source of infection that can then spread to the trunk, arms and legs (tinea corporis) or groin (tinea cruris, or jock itch). Cats, dogs and other animals are a common source of ringworm fungus, but many types can be spread between people too.
The fungus continues to spread further out while the inner area heals, forming a distinctive ring shape. Grook Da Oger
Typically, tinea spreads in a circular or oval patch, often healing in the middle so that it appears to be a red scaly ring of infection. Sometimes it can also become a fungal abscess that looks like a boil, feels boggy, and has pustules.
On the feet it can look like ringworm circles, patchy fine dry scales on the sole, blisters on the instep or a moist, red peeling area between the toes (athlete’s foot).
In the groin, it can have a scaly, red raised border and be extremely itchy.
Tinea is diagnosed by microscopic examination and laboratory culture of skin scrapings. It’s usually treated with antifungal creams, or oral antifungal drugs if it persists. It can become chronic in the warm, moist folds of the body.
Shingles
Shingles is a famously painful, blistering rash caused by the reactivation of chicken pox virus, varicella-zoster virus, usually years or decades after the original infection.
The virus lies dormant in nerves near the spine and migrates down the sensory nerve to the skin when it is reactivated, but it’s not known why the virus is reactivated. Some possible triggers are radiotherapy, spinal surgery, other infections, or cancers.
Shingles forms a painful, blistered red rash along the line of a sensory nerve. Fisle
Shingles starts with pain in the skin that is often described as burning or stabbing, followed in one to three days by a rash of raised red bumps that become blisters and then crust over. The rash is usually confined to a narrow arc of skin, along the sensory nerve that was harbouring the virus.
Patients often have a fever, headache and swollen lymph nodes. Recovery takes two to four weeks but the pain can persist after the rash has healed, called post-herpetic neuralgia.
If it’s caught within three days of onset, antiviral medication can reduce the severity of symptoms and length of the infection. Otherwise, treatment consists of powders or solutions to dry out the rash, as well as pain relief and rest.
Australians aged over 70 are eligible for a free zoster vaccine, which reduces the risk of shingles by half.
This article is part of our series about skin: why we have it, what it does, and what can go wrong.
Our skin is a big deal – literally. It’s the largest organ in the body and one of the most complicated. It has many roles in the maintenance of life and health, but also has many potential problems, with more than 3,000 possible skin disorders.
Not only does the skin hold everything in, it also plays a crucial role in providing an airtight, watertight and flexible barrier between the outside world and the highly regulated systems within the body. It also helps with temperature regulation, immune defence, vitamin production, and sensation.
The skin is unique in many ways, but no other organ demands so much attention and concern in both states of disease and health. There is a huge focus on skin health, with fierce competition to have glowing, clearer, healthier, younger and fresher skin. And this focus can cause secondary problems with self-esteem and mental health.
So, what exactly is our skin meant to do and how does it impact our life?
The structure of the skin
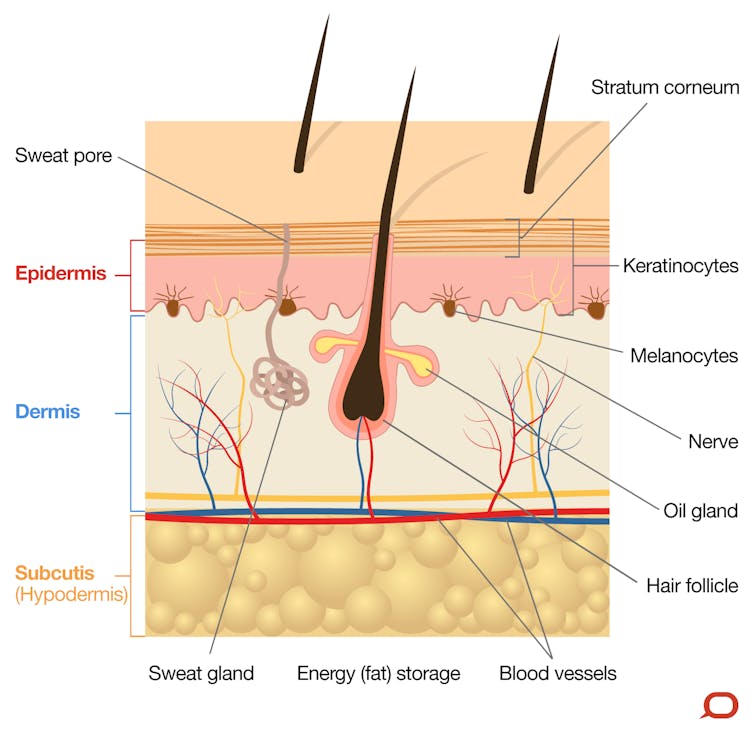
The skin is divided into three layers known as the epidermis, dermis and subcutis. These layers are well defined but together they allow the skin to function effectively.
The epidermis is the outermost, cellular layer of the skin which varies in thickness depending on the body site. On average it’s less than half a millimetre thick. The epidermis resembles a “brick wall” of cells known as keratinocytes, which are bound tightly together and act to prevent free movement of moisture, pathogens and chemicals into or out of the body.
Keratinocytes replicate from the basal layer and work their way up to the outer surface (known as the stratum corneum) over a period of about 28 days. Once they reach the surface the tight bonds between them break apart and they are shed.
Other than keratinocytes, pigment-producing cells known as melanocytes and immune cells known as Langerhans cells also exist within the epidermis. Melanocytes inhabit the basement membrane, at the base of the epidermis and produce a pigment known as melanin both innately (giving the skin its natural colour), and in response to ultraviolet light (UV) exposure (giving the skin a sun tan).
The melanin is a brown pigment that is taken up into the overlying keratinocytes. This pigment will then absorb UV light (from the sun) when it hits the skin, thereby protecting the basal calls underneath from UV damage.
The epidermal cells also develop hair follicles, sweat glands and sebaceous (oil) glands which extend down into the layer below known as the dermis. The small ducts from each of these glands open onto the skin surface. Sweat and sebum (oil) provide an antibacterial and protective barrier on the skin.
The dermis lies beneath the epidermis and is 20-30 times thicker. It’s made up of a dense layer of fibrous (collagen) and elastic (elastin) tissue. The dermis gives the skin its integrity, strength and elasticity; and houses blood vessels, glands and hair follicles, as well as nerves and their receptors.
Beneath the dermis lies the subcutis (also known as the hypodermis), a specialised layer of adipose (fat) and fibrous tissue. The thickness of this layer varies dramatically depending on the site and a person’s body shape and weight. It cushions the body from external trauma, insulates from the cold and stores energy (fat).
We pay more attention to the health of our skin than perhaps any other organ. Unsplash/Isabelle Winter
The function of the skin
The extraordinary array of functions performed by healthy skin is still coming to light. The basic day-to-day functions include:
Working as a barrier – protecting against water loss as well as physical and chemical injury, and bugs
Helping us fight off bugs, allergens, toxins and carcinogens via the parts of our immune system that exist in our skin
Regulating our temperature by dilating and constricting our blood vessels near the skin surface, controlling the transfer of heat out of the body. Temperature is also regulated by evaporative cooling due to sweat production and by the insulating effect of erect hairs on the skin surface. Heat loss is also affected by the insulating layer of subcutaneous fat
Giving us the sense of touch _ providing interaction with physical surroundings, allowing all fine and gross motor activities and allowing pleasurable and sexual stimulation
Beauty and physical attraction – the quality and condition of the skin greatly contributes to the perception of health, wellness, youth and beauty.
What is normal skin and how can you optimise it?
Normal healthy skin has many important roles and thus should be treated with care and respect. Many people only start focusing on the skin once there is an abnormality or at least a perceived problem.
Common concerns include dryness, sensitivity, oiliness, congestion, wrinkles, sun damage and signs of ageing. Although these states are all within the spectrum of normal functional skin, they may be considered problematic if severe or undesirable.
You only get one skin. Don’t do this to it. Unsplash/Maciej Serafinowicz
Normal, healthy skin that is not exposed to excessive physical or environmental insults may not require any specific care or protection, but for those who want to optimise or improve their skin, some basic steps can make a big difference.
The key to skin care is consistency and routine, and it can take time to appreciate the changes. A basic regime of daily protection from excessive UV radiation, protection from excessive irritation and drying (by avoiding drying soaps, excess water or irritating chemicals) and aiding of the skin’s barrier properties (using a moisturising protective layer) will result in noticeable improvement in almost all skin.
Switching and changing products and routines is usually counterproductive and will prevent you from seeing expected improvement in time. It’s worth looking after your skin, as you’ll wear it every day for the rest of your life.
Katin chief says previously expelled Christians will be shot if they return.
DUBLIN, November 9 (CDN) — Officials in Katin village, southern Laos have ordered six more Christian families to renounce their faith or face expulsion in early January, advocacy group Human Rights Watch for Lao Religious Freedom (HRWLRF) reported today (Nov. 9).
The Katin chief and the village religious affairs officer, along with local security forces, recently approached the six families with the threat after having expelled 11 Christian families, totaling 48 people, at gunpoint last January. The six families now under threat had become Christians since the January expulsion.
The eviction last January followed months of threats and harassment, including the confiscation of livestock and other property, the detention of 80 men, women and children in a school compound and the death by asphyxiation of a Christian villager. (See http://www.compassdirect.org, “Lao officials Force Christians from Worship at Gunpoint,” Feb. 8.)
Immediately after the expulsion, two more families in Katin village became Christians despite the obvious risk to their personal safety, according to HRWLRF. The village chief allowed them to remain in Katin but warned all villagers that their own homes would be “torn down” if they made contact with the expelled Christians.
In the following months, the expelled villagers suffered from a lack of adequate shelter, food and water, leading to eye and skin infections, diarrhea, dehydration and even the death of one villager. Katin authorities also denied Christian children access to the village school. (See http://www.compassdirect.org, “Christians Expelled from Village Suffer Critical Illnesses,” May 14.)
District officials in early May gave the Christians permission to return to Katin and take rice from their family barns to prevent starvation, said another source on condition of anonymity. Some families then tried to cultivate their rice fields to avoid losing them completely, but the work was extremely difficult as authorities had confiscated their buffaloes, essential to agriculture in Laos.
Threat to Shoot
In July, officials from the Saravan provincial headquarters and the Ta-oyl district religious affairs office met with the evicted families in their shelters at the edge of the jungle and encouraged them to return to Katin, HRWLRF said.
The Christians agreed to return under five conditions: that authorities designate a Christian “zone” within Katin to avoid conflict with non-believers; that all forms of persecution end; that their children return to school; that Christians must be granted the right of burial in the village cemetery; and that the village award compensation for six homes destroyed in the January eviction.
When higher-level officials approached Katin leaders with these terms, village officials and local residents rejected them, insisting that they would only allow the Christians to return if they gave up their faith. The higher officials invoked Decree 92, a law guaranteeing the rights of religious minorities, but village heads said they would shoot every Christian who returned to Katin.
Shortly after this discussion took place, a further four families in Katin became Christians, according to HRWLRF.
A communist country, Laos is 1.5 percent Christian and 67 percent Buddhist, with the remainder unspecified. Article 6 and Article 30 of the Lao Constitution guarantee the right of Christians and other religious minorities to practice the religion of their choice without discrimination or penalty.
Muslims said to use mistaken identity to stop activities of Christian who refused to recant.
DHAKA, Bangladesh, August 27 (CDN) — A Christian convert from Islam was falsely arrested for cattle theft last weekend in a bid by influential Muslims to stop his Christian activities, area villagers said.
Day laborer Abul Hossen, 41, was arrested on Saturday (Aug. 21) for alleged cattle theft in Dubachari village in Nilphamari district, some 300 kilometers (180 miles) northwest of the capital, Dhaka.
Christian villagers told Compass that Hossen was the victim of “dirty tricks” by influential Muslims.
“There is another Abul Hossen in the village who might be the thief, but his father-in-law is very powerful,” said Gonesh Roy. “To save his son-in-law, he imputed all the blame to a different Abul Hossen who is a completely good man.”
Hossen, who converted to Christianity from Islam in 2007, has been very active in the community, and Muslims are harassing him with the charge so his ministry will be discredited and villagers will denounce his faith, Roy said.
“If he can be accused in the cattle theft case, he will be put in jail,” Roy said. “He will be a convicted man, and local people and the believers will treat him as a cattle thief. So people will not listen to a thief whatsoever.”
Some 150 villagers, about 20 percent of them Christian, went to the police station to plea for his freedom, he and other villagers said.
Sanjoy Roy, a lay pastor with Christian Life Bangladesh, told Compass that Hossen was a fervent Christian and that some Muslims have been trying to harass him since his conversion.
“They are hoping that if he is embarrassed by this kind of humiliation, he might not witness to Christ anymore, and it will be easy to take other converted Christians back to Islam,” Sanjoy Roy said. “He is a victim of dirty tricks by some local people.”
Hossen was baptized on June, 12, 2007 along with 40 other people who were raised as Muslims. Of the 41 people baptized, only seven remained Christian, with villagers and Muslim missionaries called Tabligh Jamat forcing the remaining 34 people to return to Islam within six months, sources said.
Local police chief Mohammad Nurul Islam told Compass that officers had arrested a cattle thief who confessed to police that his accomplice was named Abul Hossen.
“Based on the thief’s confessional statement, we arrested Abul Hossen,” said Islam. “There are several people named Abul Hossen in the village, but the thief told exactly of this Abul Hossen whom we arrested.”
Hossen denied the allegation that he was involved in cattle theft, Islam said.
“Hossen is vehemently denying the allegation, but the thief was firm and adamantly said that Hossen was with him during the theft,” he said. “Then we took Hossen on remand for three days for further inquiry.”
A former union council chairman who is Muslim, Aminur Rahman, also told Compass that Hossen was a scapegoat.
“He is 100 percent good man,” said Rahman, who also went to the police station to plea for Hossen’s freedom the day after his arrest. “There are two or three people named Abul Hossen in the village. Anyone of them might have stolen the cattle, but I can vouch for the arrested Abul Hossen that he did not do this crime.”
Whether Hossen is a Christian, Muslim or Hindu should not matter in the eyes of the law, Rahman said.
“He is an innocent man,” he said. “So he should not be punished or harassed. That is why I went to police station to request police to free him.”
Local government Union Council Chairman Shamcharan Roy, a Hindu from Lakmichap Union, told Compass that Hossen was not engaged in any kind of criminal activities.
“In my eight years of tenure as a union council chairman, I did not find him engaged in any kind of criminal activities,” said Shamcharan Roy. “Even before my tenure as a chairman, I did not see him troublesome in the social matrix.”
Immediately after Hossen’s arrest, Shamcharan Roy went to the police station and requested that he be freed, he added.
“I was under pressure from local people to free him from custody – more than 100 villagers went to the police camp, getting drenched to the skin in the heavy downpour, and requested police to free him,” Shamcharan Roy said. “Police are listening to a thief but are deaf to our factual accounts about Abul Hossen.”
In July 2007, local Muslims and Tabligh Jamat missionaries gathered in a schoolyard near the homes of some of the Christians who had been baptized on June 12, a source said. Using a microphone, the Muslims threatened violence if the converts did not come out.
Fearing for their lives, the Christians emerged and gathered. The source said the Muslims asked them why they had become Christians and, furious, told them that Bangladesh was a Muslim country “where you cannot change your faith by your own will.”
At that time, Hossen told Compass that Muslims in the mosque threatened to hang him in a tree upside down and lacerate his body with a blade. Hossen said the Muslims “do not allow us to net fish in the river” and offered him 5,000 taka (US$75) and a mobile phone handset if he returned to Islam.
“But I did not give up my faith, because I found Christ in my heart,” Hossen told Compass in 2007. “They threatened me with severe consequences if I do not go back to Islam. I said I am ready to offer up my life to Christ, but I won’t renounce my faith in Him.”

























You must be logged in to post a comment.